Escalation paththresholds: configurable
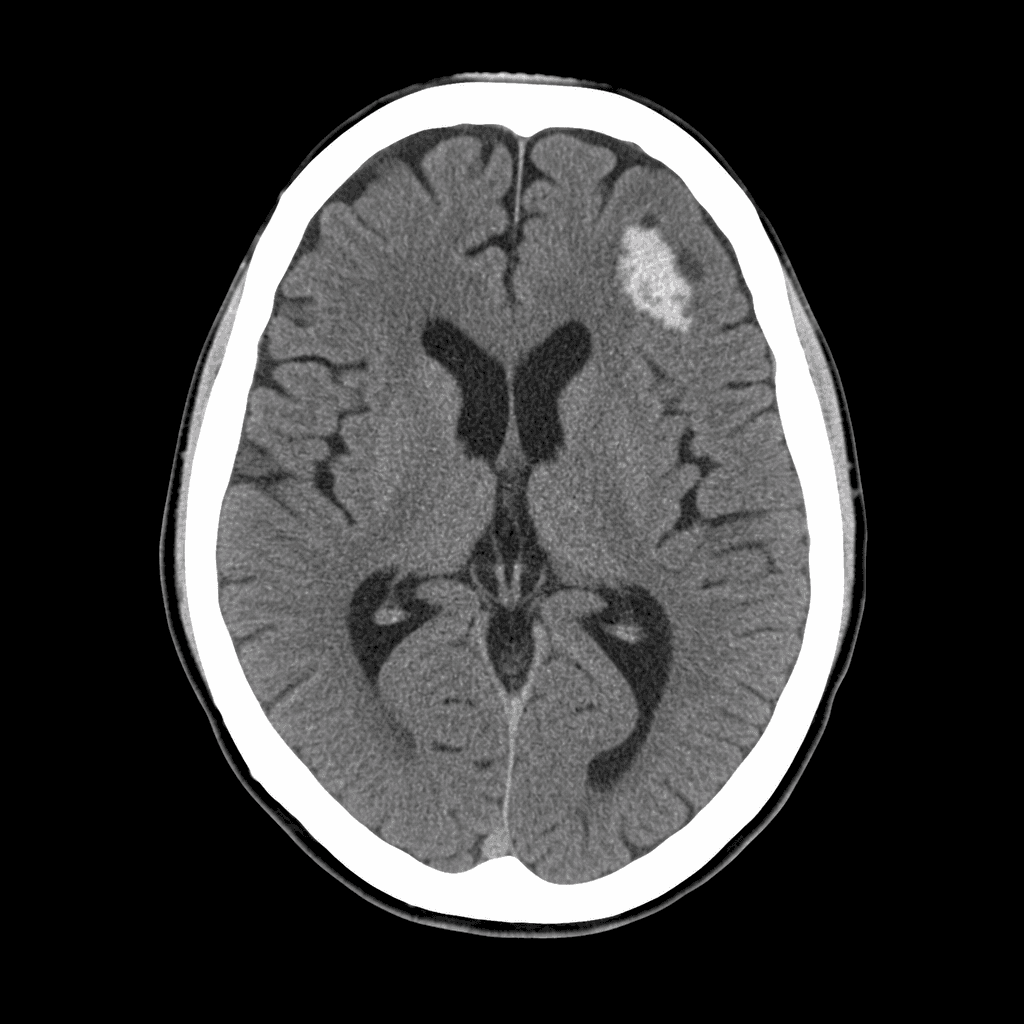
CT-0491
STAT
CT-0487
STAT
CT-0489
Urgent
CT-0485
Urgent
US-0483
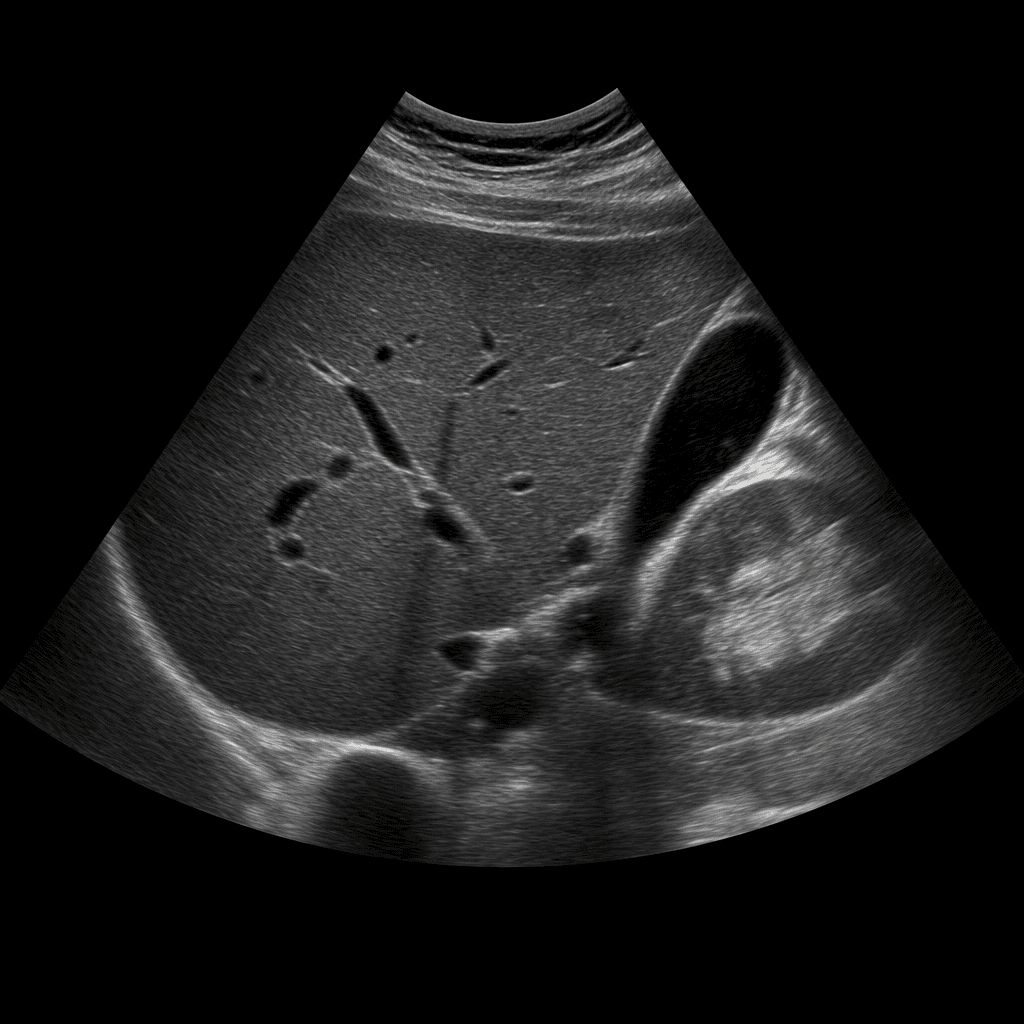
Routine
→ STAT studies routed to on-call neuroradiology
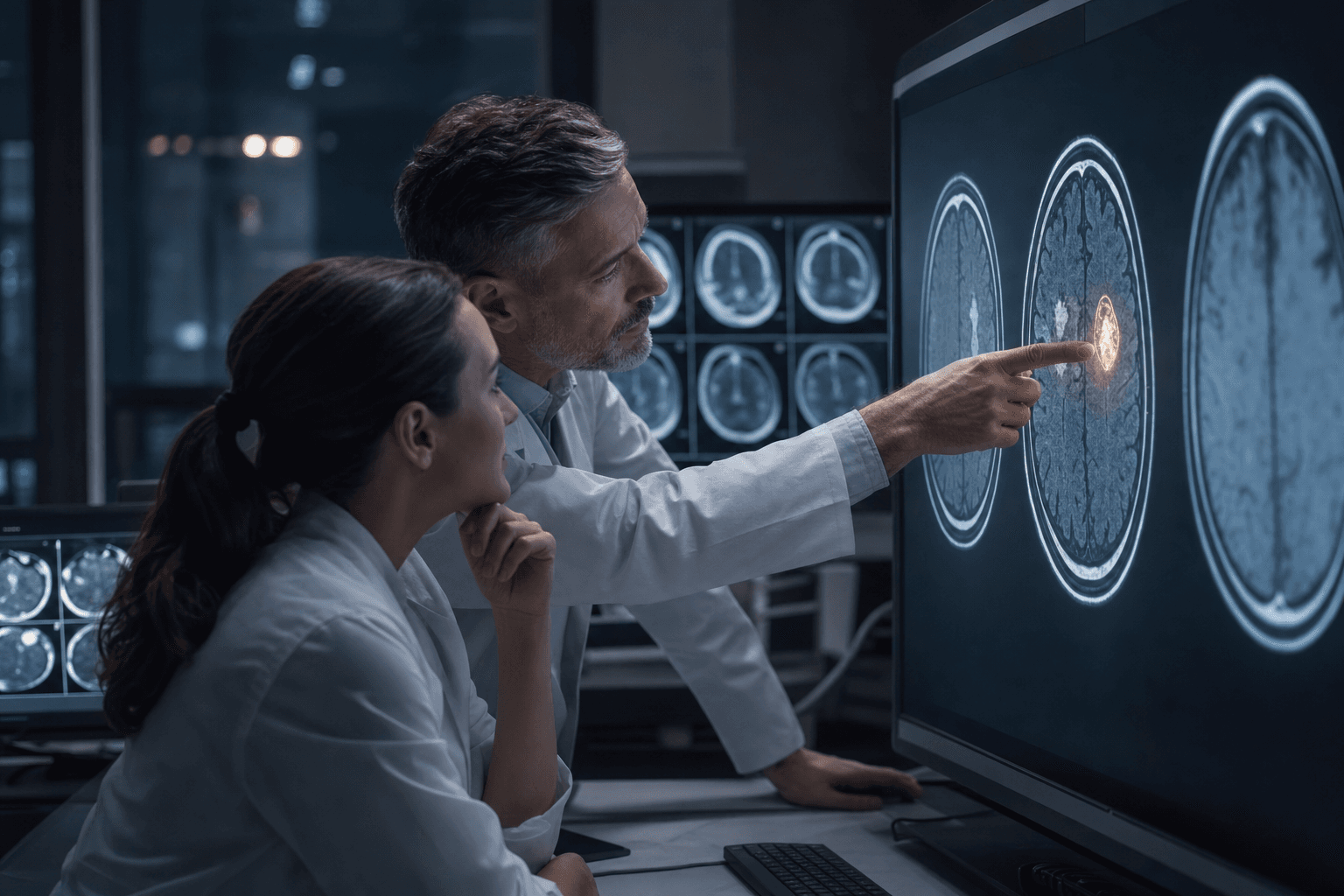
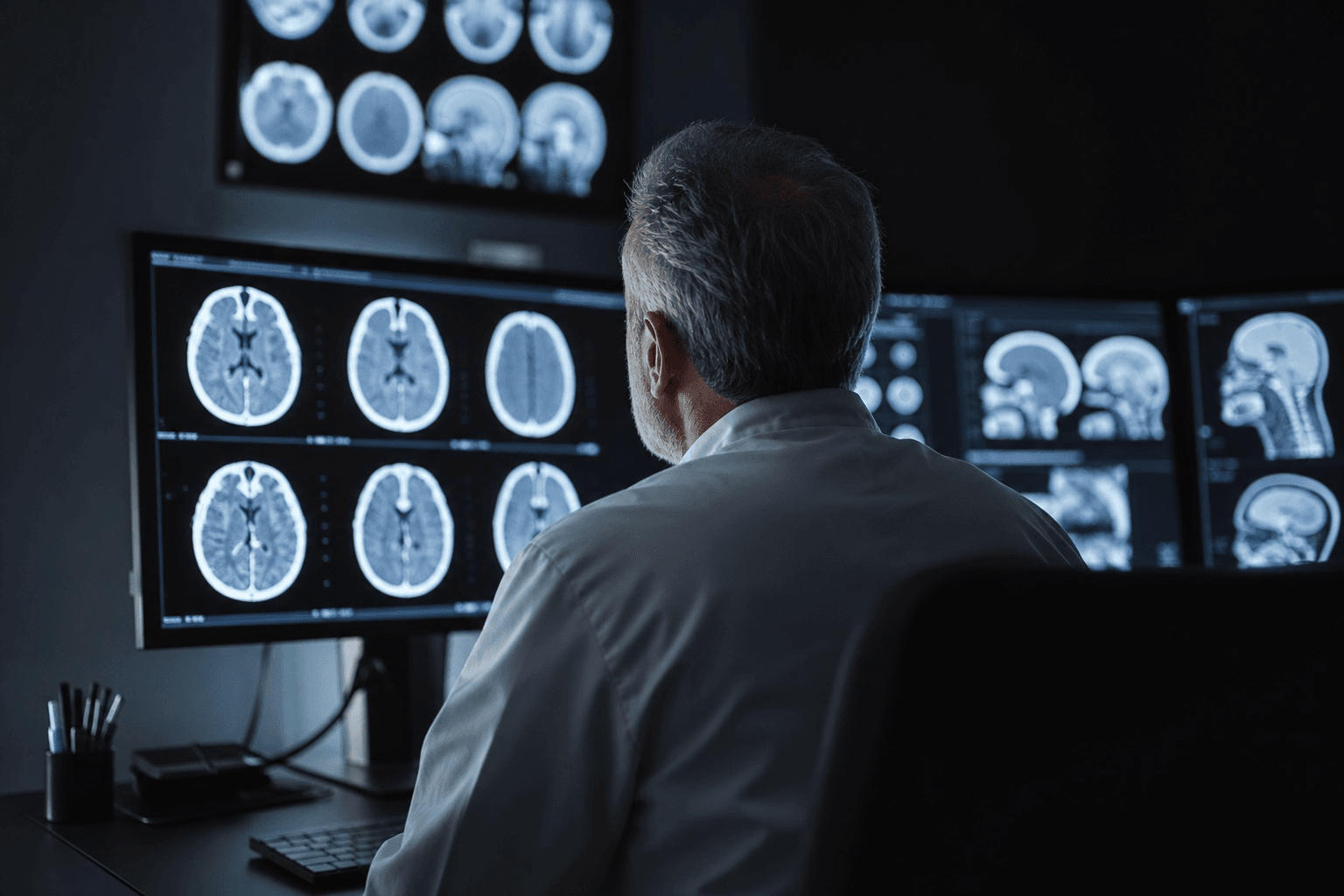
01 · Critical Finding Triage
The queue reorders itself around urgency
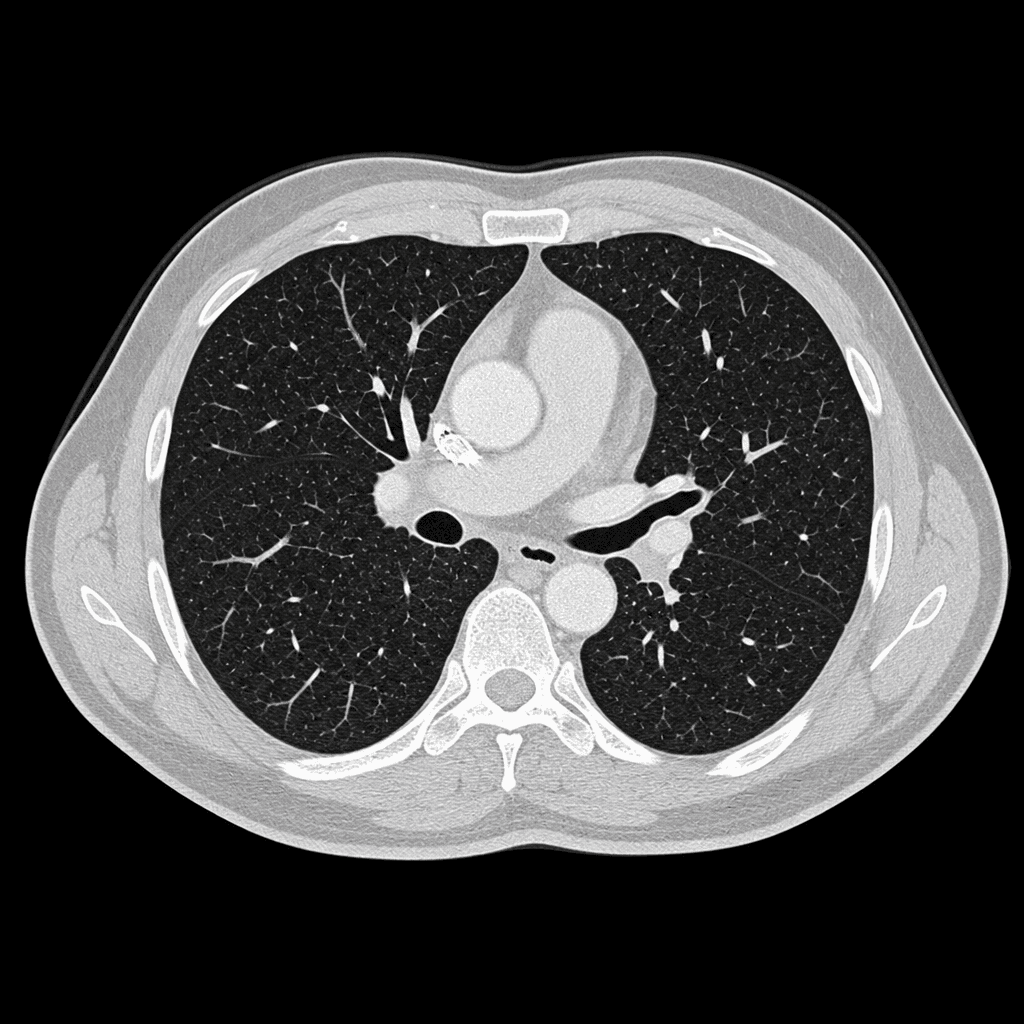
AI models surface time-sensitive findings — hemorrhages, mass effects, critical fractures — and escalate them to the top of the reading queue before a radiologist even opens the study.
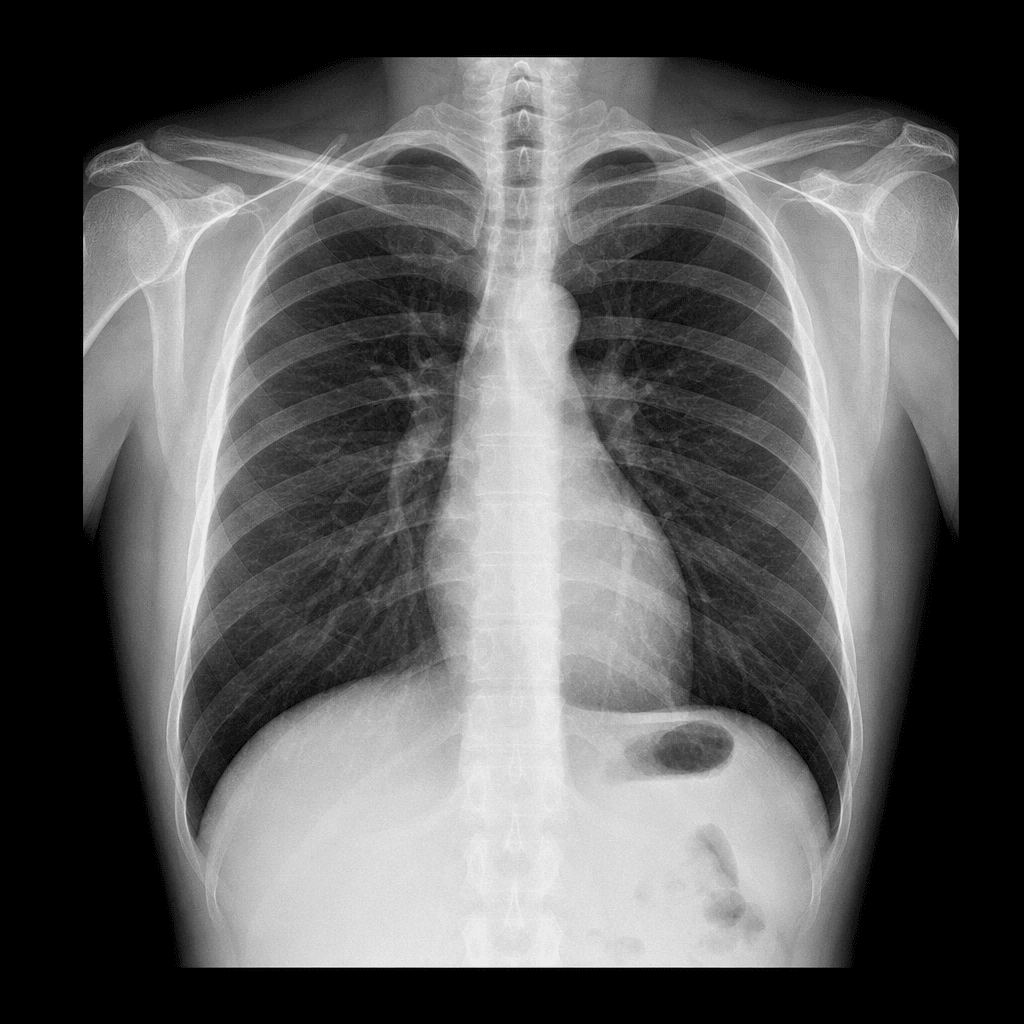
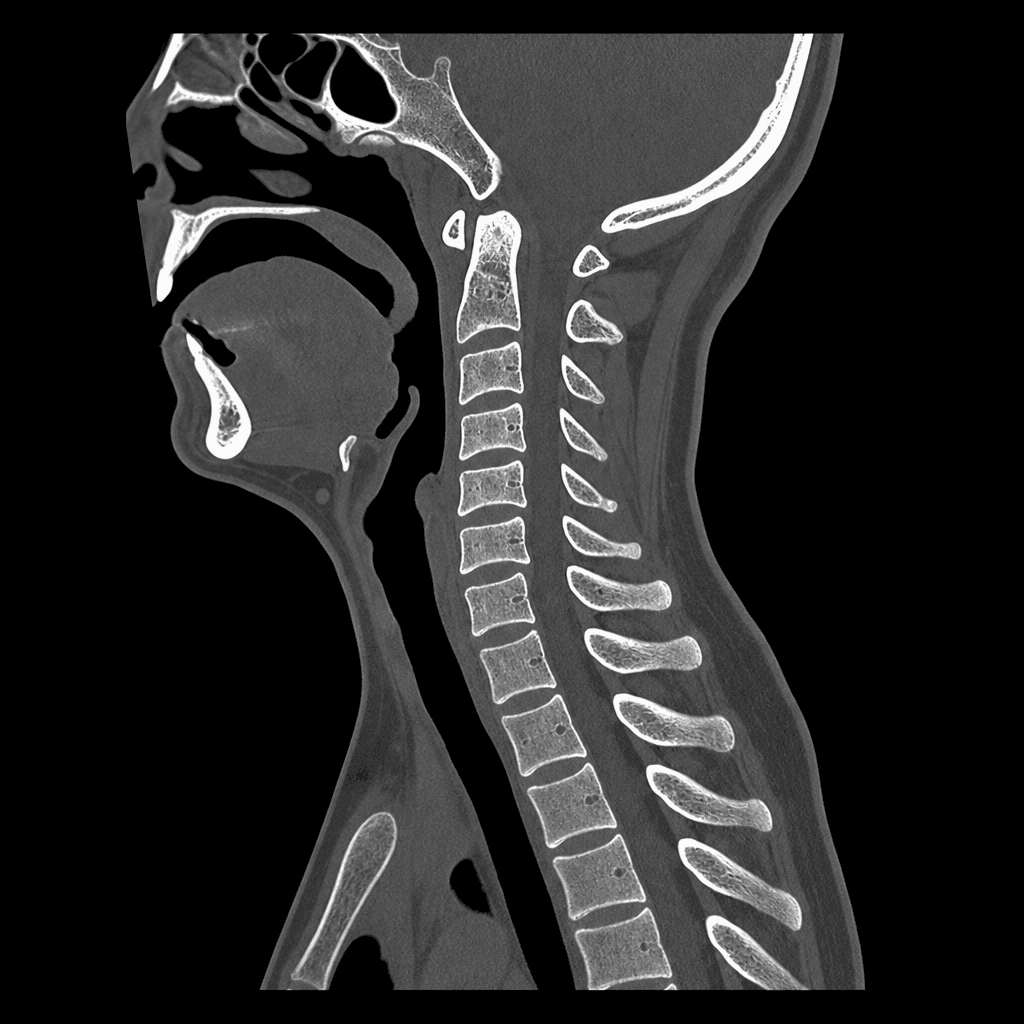
Runs on CT Head, Chest, and C-Spine studies as they arrive, with configurable escalation thresholds and automated routing to on-call staff.
CT hemorrhage triageCT Head / Chest / C-SpineWorklist escalation